India has become remarkably good at moving things across distance.
Money moves instantly through UPI. Groceries arrive at doorsteps in minutes. Government benefits reach villages digitally. Yet, there is surprisingly one simple thing that still struggles to reach millions of Indians: a basic pair of glasses.
As more Indians enter their late 30s, presbyopia — the age-related decline in near vision becomes common. It develops gradually, many people simply adapt to the problem rather than seek help. The irony is that the solution is neither expensive nor complicated. In most cases, a simple pair of near-vision glasses can restore clear sight almost instantly.
So why do millions continue to live with blurry near vision? Why is awareness still low, and why do so many people remain unreached by something so simple?
The challenge is not the lack of a solution. It is finding effective ways to make vision screening and near vision glasses accessible, affordable, and trusted within communities.
Three ways to take spectacles to the last mile
Unlike most healthcare interventions, near-vision screening is relatively simple to deliver: a vision chart, measuring tape, trial lenses, and basic training are often enough to identify and correct impairment at the household level. This simplicity makes community-based delivery both feasible and scalable.
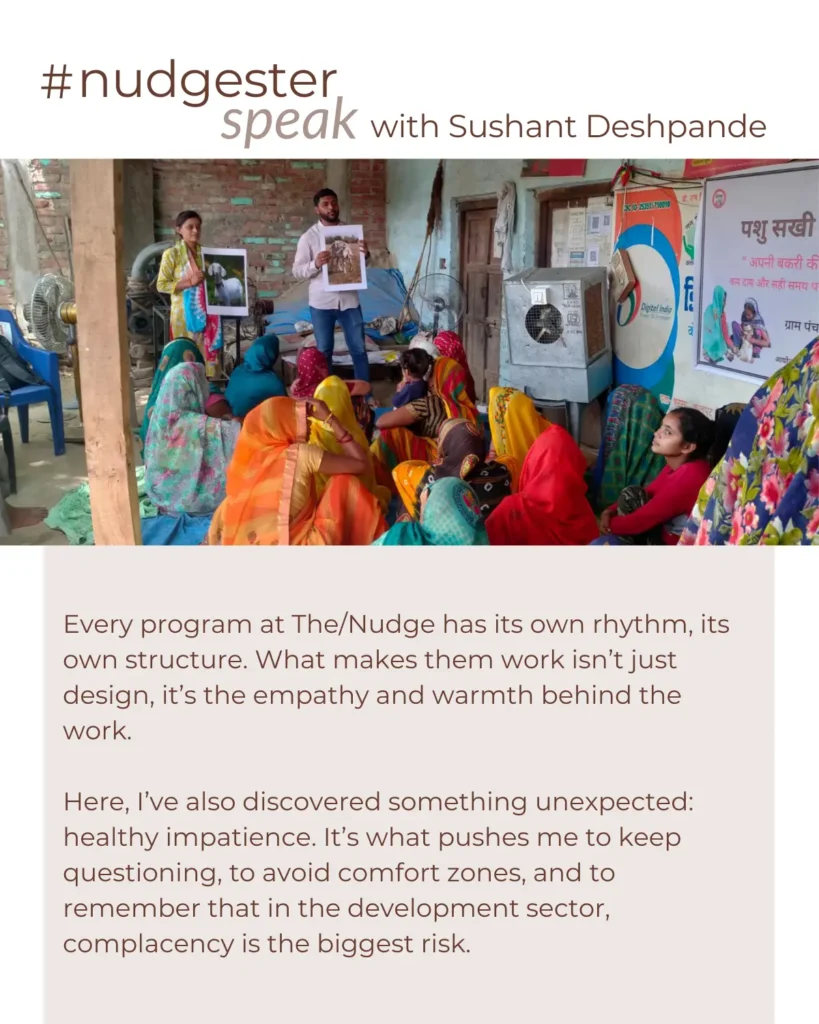
The InSight program, implemented by The/Nudge, is testing exactly this. Rather than relying on eye camps, hospital outreach, or optometrist visits, the program is building the capacity of three types of community cadres to screen for near-vision impairment and distribute near vision glasses: Accredited Social Health Activists (ASHAs), Community Resource Persons (CRPs), and Community Entrepreneurs.
Here is what we have learned about each of them.
1. Accredited Social Health Activists (ASHAs)
India has seen several efforts in the past that have meaningfully bridged the last mile. Remember the “Do Boond Zindagi Ke” campaign that came to symbolize the country’s fight against polio? It is often cited as a public health success —vaccinating over 170 million children annually, mobilizing more than a million workers, and eventually eliminating polio from the country.
ASHA workers (then Anganwadi workers) became the quiet backbone of this effort. They went door to door, spoke with families, built trust over time and eventually turned polio vaccination from a medical intervention into a sustained behavioural change.

India has 1 million ASHAs embedded in villages across the country. An ASHA is not a visiting health worker. She lives in the village. She is trained, registered, and recognised by the government. She is a neighbour, often a relative, almost always the first health contact for the households on her list. The reach is already there. The relationship is already there. When an ASHA worker tells a woman in her forties that her blurred vision can be corrected with a simple pair of glasses, the message carries trust and credibility.
Karnataka’s ASHA Kirana program demonstrated it at scale: approximately 7,500 ASHA health workers trained in door-to-door visual acuity testing successfully reached 5.6 million people in its first phase.
2. Community Resource Persons (CRPs)
India has approximately 90.9 lakh Self Help Groups under the Deendayal Antyodaya Yojana – National Rural Livelihoods Mission (DAY-NRLM), covering over 10 crore women households as of early 2025. These are groups of 10–20 women, drawn from the same village or neighbourhood, who meet regularly, typically once a fortnight or monthly to deposit savings, access credit, discuss livelihoods, and increasingly take on a widening range of community functions.
At the heart of this network is a cadre of women known as Community Resource Persons, or CRPs. Drawn from within SHG networks and selected for their track record, initiative, and peer standing, CRPs are trained to facilitate group functioning, support financial inclusion, and lead livelihood promotion activities in her village. They are sometimes referred to as Pashu Sakhi, Krishi Sakhi, Bank Sakhi etc. appointed under NRLM model as trusted advisors who are for creating pathways for sustainable livelihoods. A CRP is generally an active community member often from similar economic circumstances, who has navigated the system and is now helping others do the same.
What makes CRPs a powerful channel for vision care is not health expertise, but regular human connection. SHG meetings happen every fortnight — women are already gathered, trust already exists, and conversations happen naturally. Unlike ASHAs, who speak as health workers, CRPs speak as peers who understand the same daily challenges. That peer credibility can make CRPs an effective non-health arm of vision care.
3. Community Entrepreneur
A simple pair of near vision glasses costs around ₹200–500 in an optical shop. The problem it solves is nearly universal among adults over 35. And our field experiences consistently show that participants who benefit from glasses are willing to pay for a pair.
But, the real challenge is access. For many villagers, the nearest optometrist or optic shop is over 50 km away, often requiring an entire day of travel, loss of wages, and additional expenses for screening and purchasing glasses. The issue is not creating demand from scratch, but solving the last-mile problem: getting the right glasses to the right person.

This is precisely what a well-supported entrepreneur can do. She is local, trusted, and motivated — someone willing to build a livelihood around a problem her own community faces every day. With training in near-vision screening and a starter kit of trial lenses and stock, she becomes an eye care professional. Selling even 20 pairs a month can generate up to ₹6,000 a month. Our experiences from the entrepreneurship model in Tamil Nadu have shown encouraging results, with entrepreneurs building steady clientele through word of mouth once the first few satisfied customers spread the word. Read more about the entrepreneurship model here.
Conclusion
Some problems do not require a technological breakthrough. Community networks already hold immense potential to strengthen last-mile vision care access in India because they are built on trust, familiarity, and local presence. At the same time, expanding these networks must be approached thoughtfully, with an understanding of the realities frontline workers navigate every day. ASHAs already shoulder responsibilities across maternal health, nutrition, and immunisation; CRPs support multiple self-help groups across villages, and for an entrepreneur model to work out, it would require careful selection and realistic unit economics. Any successful vision care program must therefore view frontline workers not simply as delivery channels, but as partners operating within real constraints of time, workload, and mobility. Strengthening community-based vision care will depend not only on leveraging these networks, but also on supporting them with adequate training, sustainable incentives, and realistic implementation models.